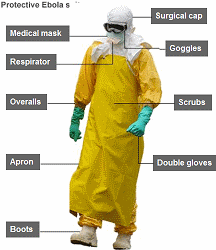
Imagine a patient admitted to a hospital ward in the UK who has been properly trained in their own safety protection. They will have had simulation training for their hospital episode to rehearse how to check that drugs and procedures are appropriate and correct. They will have been trained to communicate effectively in ward rounds and consultations. They will have a hospital buddy who keeps a close eye out for them and picks up early warning signs of problems. They will have taken suitable precautions to protect themselves from acquiring hospital infections. They may well look something like this:
One of the most fascinating aspects of working in Sierra Leone on the Ebola emergency was the complete obsession with safety. We had nine days of army training to ensure that the repetitive drills of donning and doffing were part of our autonomic nervous system. We had detailed simulation trained in a full mock-up of an Ebola hospital in a giant warehouse in Yorkshire so that we could gain experience at taking toxic blood, putting in cannulas and dealing with emergency situations in the high risk red zone of an Ebola ward. We had training manuals and SOPs for every situation; close observation and feedback using CCTV; small group work to improve our technique; army sergeants to shout at us when we got things wrong. We also learnt to work closely in pairs so that all the time we were in the red zone we had our own ‘Ebola buddy’ to look out for us and provide help and support.
There was one big and very noticeable difference between our safety training for Ebola and our safety training in the NHS. In the UK safety is, superficially at least, all about the patient – communication, design and training to reduce medication errors, pick up deteriorating patients, avoiding wrong site surgery. In Sierra Leone it was all about the professional – communication, design and training to reduce infection risk for Ebola.
It would be lovely to think that our focus on the patient in the UK is because we are putting them first. However what we are really doing is building fragile defences to try to mitigate the inevitability of our slips, lapses, trips and fumbles of human behaviour and the inherent flaws in the designs of our health systems.
The Ebola response shows how we can really do safety properly if we put our minds to it. And the reason for this cultural prioritisation of safety? It is because if something goes wrong in an Ebola hospital then the health care worker dies, not the patient. One of the reasons why airline pilots take safety so much more seriously than doctors is that they are the first ones to die when the plane flies into the side of a mountain.
Ebola provides a great illustration of what we can really do if we are serious about improving safety, when it’s us not the patients who are in the firing line of harm but us. The ever present threat of infection and death from Ebola provided an urgency that may be less immediate in the NHS, but we know from the 10% of patients who experience hospital errors, is just as real.
We are never going to send patients for army training or get them to wear biohazard suits, but we can help to improve our safety training and systems by putting ourselves in our patients shoes – a mind-set of ‘safety reciprocity’ where we are voodoo dolls for our patients and everything we do is framed by the belief that the harm we cause will harm ourselves.