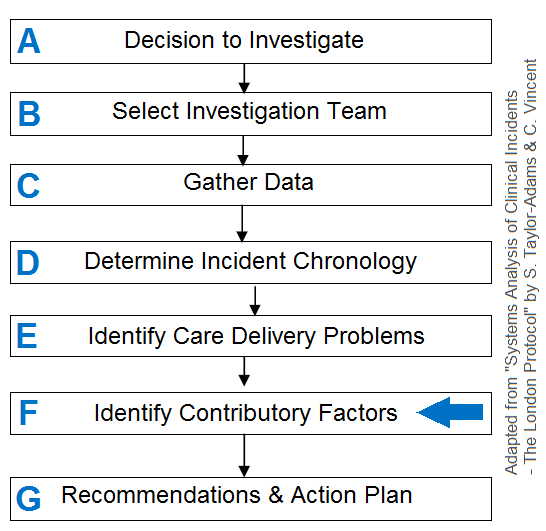
Human factors in patient safety incidents
Patient safety incidents (PSIs) are common and can lead to fatal outcomes. Effective investigation of PSIs is essential to optimize learning and take action to prevent further incidents occurring. Good practice in incidents investigation has been described by the NPSA in the London Protocol. A key step in this protocol is the identification of all contributory factors. The Clinical Human Factors Group also recommends effective contributory factor analysis as part of serious incident investigation.
The research behind the Yorkshire Contributory Factors framework
In 2012, a systematic review of 83 research studies focusing on the causes of hospital patient safety incidents was conducted. The result of this piece of work is the first evidence-based framework of accident causation in hospitals: the Yorkshire Contributory Factors Framework.
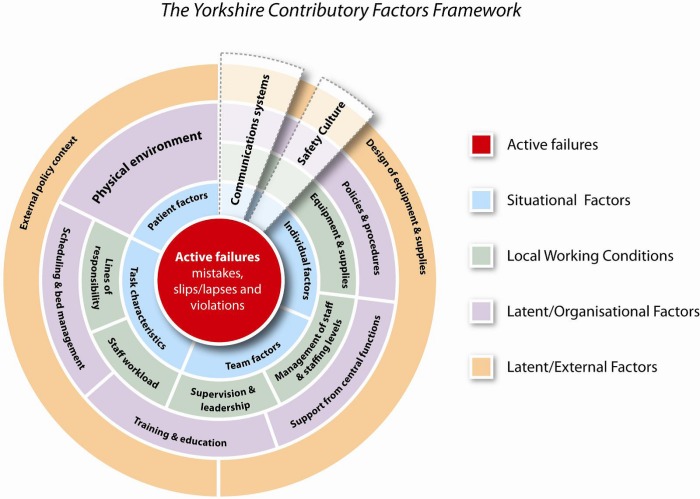
The Yorkshire Contributory Factors Framework is a tool which has an evidence base for optimizing learning and addressing causes of patient safety incidents by helping clinicians, risk managers and patient safety officers identify contributory factors of PSIs. Incidents that occur in a hospital setting have been well studied and all contributory factors have been mapped. Download the supporting research here.
An adapted version for clinical practice
Based on this research, a team of practicing clinicians and risk managers, with human factors experts has adapted the evidence to a pragmatic 2 page framework that can be downloaded by clicking on the image below.
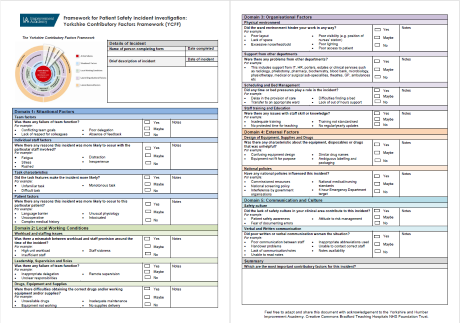
The document suggests questions that you might want to ask of those involved in the incident. The underlying aim of this tool is not to ignore individual accountability for unsafe care, but to try to develop a more sophisticated understanding of the factors that cause incidents. These factors can then be addressed through changes in systems, structures and local working conditions. Finding the true causes of patient safety incidents offers an opportunity to address systemic flaws effectively, for the benefit of all our future patients.
![]()