Historically, the commitment by health care professionals to ‘first do no harm’ has led to the absence of interventions that may cause adverse outcomes. This clinical approach links to the Hippocratic Oath which states, “to abstain from doing harm” (Luxford, 2016). Although started in healthcare, the same applies to social care. But what do we mean by: first, do no harm? In an attempt to mitigate harm and ensure patient/resident safety, we will often implement new procedures or policies, but is this adding value or perhaps making things less safe?
We have been working on a project aiming to improve the experience and safety of care home residents when attending the emergency department (ED) with paid carers. Understanding the journey and gathering perspectives of the residents and paid carers and the ED staff. We started this work after discussing with some ED colleages the value paid carers can and do bring when escorting residents to the ED. We then spoke to some care homes colleagues who related some shocking experiences. For example, in a focus group with senior carers, “people talk condescending to us and to the service users, some service users sit there looking like ‘why are you talking to me like that’.” It left us thinking what can we do to make this better?
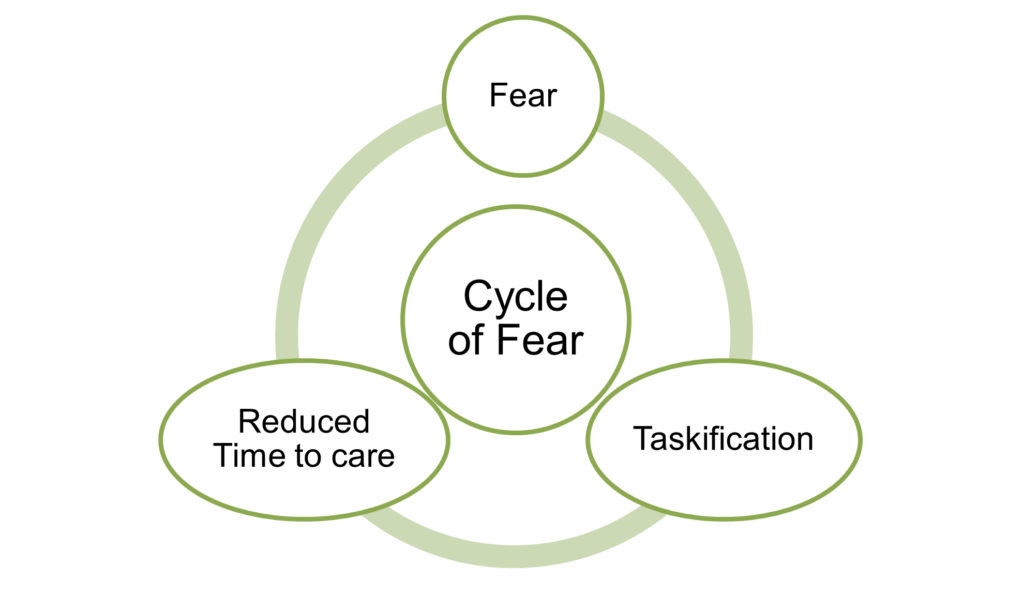
The Oxford Dictionary defines care (verb) as: “to feel that something is important and worth worrying about.” However, through this work, we found that for some colleagues at a care home, CARE was an acronym describing what they perceived as over-documentation. They described CARE as: Cover. A***. Remain. Employed, emphasising the fear experienced by staff resulting in over-documentation often linked to safeguarding. Indeed, staff felt that safeguarding was often used as a threat against them and as a result, they would over-document everything to C.A.R.E. One example was when a new resident is admitted, it could take a carer up to twelve hours to complete their documentation, taking away from the caring part of their job; ‘taskification’ of care. See Figure One.
For the registered nursing staff, there was fear in having their PIN removed due to things out of their control, sometimes leading to defensive behaviours. For example, fear of safeguarding leading to extra calls to telemedicine when they had the skills and knowledge to manage the situation themselves. A tick box exercise that took their time away from care with no benefit to the resident.
Carers also expressed fear of attending the ED with a resident due to feeling ‘attacked by questions’ and ‘scared of doing the wrong thing’, undeniably, there was a profound absence of psychological safety. In short it was a sense of a fear leading to extra tasks, ultimately resulting in less time for care for residents.
Research by Halligan et al. (2023), found that many patient safety practices were deemed as low value care, including duplication, and paperwork. Indeed, paperwork was frequently mentioned by participants as the ‘greatest waste of time’; this was primarily due to participants describing the removal of professional autonomy and the reduction of direct patient care that paperwork caused. This resonates with our work where care home collagues are ‘overdoing’ paperwork through fear of doing wrong.
Increasing the amount of documentation could be seen as ‘clutter’; introduced to try and make things safer but ultimately making things more complicated and reducing time for care.
Figure One: Vicious cycle that staff can find themselves in
What’s next for Carers in the ED work?
- We have developed a roadmap depicting a residents’ journey to the ED; we are also working with an ED to do this same exercise and plan to feed back to each respective party.
- Our aim is to develop an improvement project with both ED and care home staff. The focus of this is contingent on the aforementioned step.
Is this something you’d like to hear more about?
- We host the Y&H Care Home Support Network for colleagues working in health & care supporting care homes. We have quarterly meetings where there is opportunity to connect with colleagues and share and learn together. If you are interested in hearing more about the network, please contact Lizzie at Elizabeth.Sweeting@yhia.nhs.uk
- Please click here to view a poster of current project findings that were presented at the Qualitative Health Research Network Conference (2024) and a roadmap, visually depicting a residents’ journey to the ED.
References
Halligan, D., Janes, G., Conner, M., Albutt, A., Debono, D., Carland, J., … & Lawton, R. (2023). Identifying safety practices perceived as low value: An exploratory survey of healthcare staff in the United Kingdom and Australia. Journal of Patient Safety, 19(2), 143-150.
Luxford, K. (2016). ‘First, do no harm’: shifting the paradigm towards a culture of health. Patient Experience Journal, 3(2), 5-8.
